

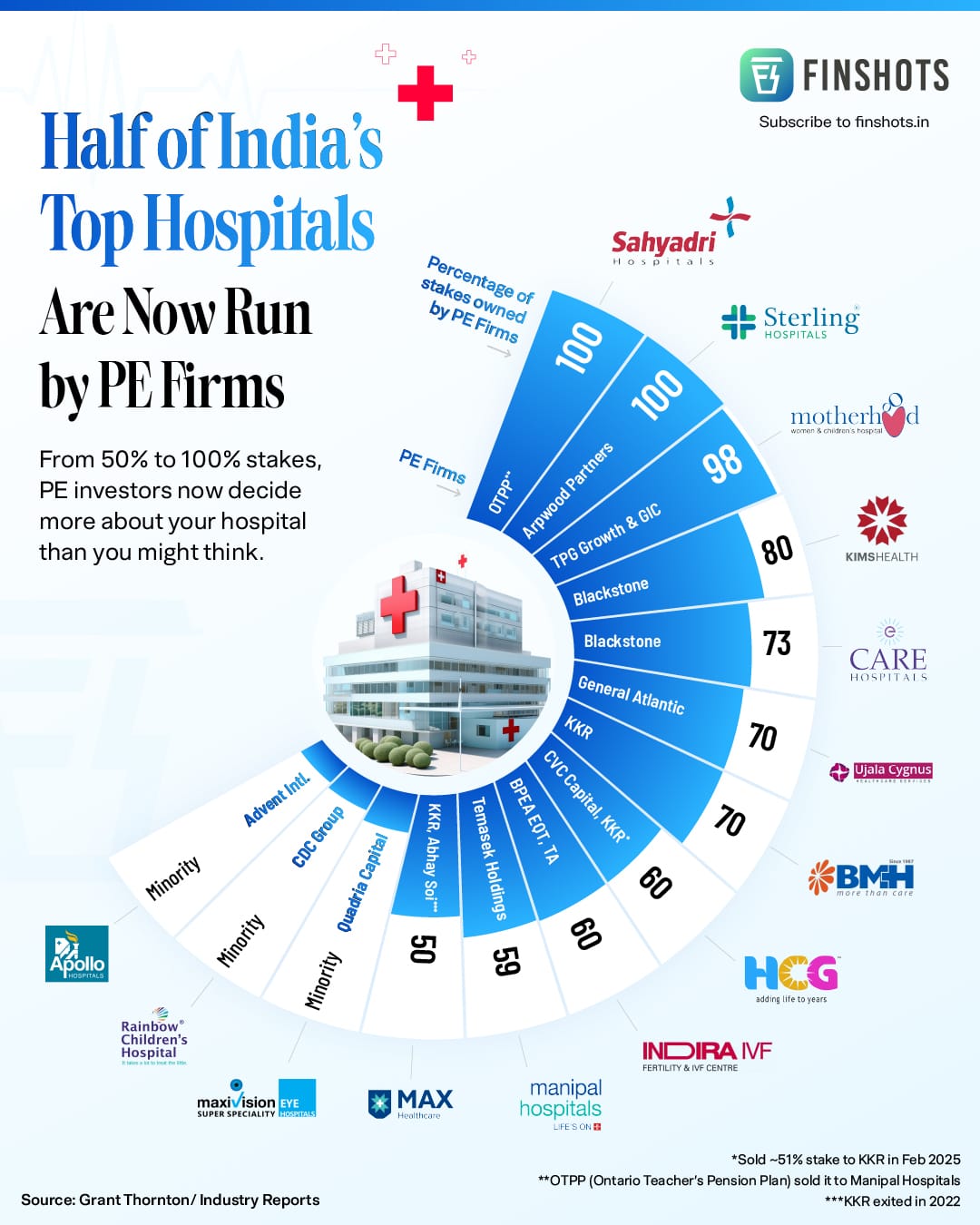
Half of India's top hospital chains are now backed by private equity. For patients, that changes more than just who owns the building — it changes how care is sold, branded, and delivered.
Why PE firms want hospitals
Private equity firms are not charities. They raise money from pension funds, sovereign wealth funds, and institutional investors, deploy it into businesses, grow the value, and exit.
At a time when PE firms globally are searching for stable, recession-proof assets, a hospital with a full bed occupancy rate and a growing middle class of patients looks very attractive.
"Hospitals have become an asset class. The question is what happens to the patient experience when the asset needs to perform."
The deals tell the story: In 2023, Temasek and TPG Capital invested $2.4 billion in Manipal Hospitals. Blackstone wrote a $700 million cheque for Care Hospitals. More recently, KKR announced a $400 million deal to acquire a controlling stake in HCG, one of India's largest cancer care networks. These are not small bets — they are strategic wagers on India's healthcare future.
When a PE firm like Blackstone or KKR takes over a hospital, the first thing that changes isn't the doctors, or the equipment, or even the prices. The first thing that changes is the language."
The language of care begins to shift. What was once designed to reassure starts getting designed to convert.
Think about the last time you received communication from a hospital — a discharge summary, a follow-up SMS, a health package brochure, a doctor's consultation note. Now ask yourself: who was that really written for?
India is in the middle of a quiet but consequential transformation. Half of the country's top hospital chains are now significantly owned by global private equity firms. Names you associate with boardrooms, not bedrooms. With portfolio returns, not patient outcomes.
The money is enormous: over $15 billion in PE and VC money has flowed into Indian healthcare over the past five years. And where large capital goes, a particular kind of management thinking follows.
Call it the McKinseyification of healthcare
From a practice to a process
There is an old distinction in medicine between a 'practice' and a 'process.' A practice is led by practitioners — doctors, nurses, clinicians — who exercise judgement, intuition, and relationships. A process is managed by systems — dashboards, protocols, KPIs — that standardise behaviour to produce predictable outputs.
For most of India's healthcare history, hospitals were practices. They were often family-run, doctor-led institutions where the founder's values — sometimes paternalistic, sometimes genuinely compassionate — set the culture. Communication was informal, often face-to-face, rooted in relationship.
When PE firms acquire a hospital, they bring operational rigour: standardised care protocols, electronic health records, and cleaner billing. These are real improvements. But they also bring the instinct to measure everything — and to optimise for what can be measured. In that world, communication is not a relationship tool; it is a conversion tool.
Hospital as Practice | Hospital as Process
|
|---|---|
Communication to care: Doctor explains the diagnosis in plain language. Follow-up is scheduled on clinical need. | Communication to convert: Digital nudges suggest premium diagnostics. Discharge paperwork includes upsell suggestions. |
Neither model is inherently better.
But they produce very different kinds of communication—and very different patient experiences.
The language of throughput
The single most important financial metric in a PE-backed hospital is ARPOB — Average Revenue Per Occupied Bed. It tells investors how much revenue the hospital generates from each bed, each night. A high ARPOB signals a premium patient mix: complex procedures, private rooms, high-value diagnostics.
Marketing, in this framework, has a clear job: to attract and retain the kind of patient that keeps ARPOB high.
This is the moment where communication quietly shifts its allegiance. It is no longer primarily designed to inform, reassure, or empower the patient. It is designed to convert, upsell, and retain.
You see it in the language of health packages — 'Executive Health Checkup,' 'Platinum Cardiac Wellness Program' — designed not around clinical need, but around aspirational identity and fear. You see it in the aggressive digital marketing of speciality procedures.
For context, Apollo Hospitals achieves an ARPOB of around ₹55,000–60,000, while value-focused chains like Narayana Health operate at ₹30,000–32,000. Marketing investments are often specifically calibrated to shift the patient mix toward higher-value procedures that push ARPOB upward.
None of this is necessarily dishonest. Most of it is probably well-intentioned. But the incentive structure has changed — and incentive structures shape communication more profoundly than intentions do.
What the research actually shows
This is not speculation. A Harvard Medical School study examining PE-acquired hospitals in the United States found that after private equity acquisition, patient experience scores worsened — more steeply than they did nationally even during the Covid-19 pandemic.
RESEARCH FINDING — HARVARD MEDICAL SCHOOL
After PE acquisition, the percentage of patients who would 'definitely recommend' the hospital decreased, while scores at comparable non-acquired hospitals improved over the same period.
Researchers noted this has broader implications: poor patient experience is associated with slower recovery, lower treatment adherence, and greater long-term healthcare utilization.
The dynamic studied in the US is now arriving in India at scale. The difference is that India has far weaker patient protection infrastructure — fewer ombudsmen, limited public data on hospital outcomes, and a patient population that is far less empowered to challenge medical authority or switch providers.
When McKinsey works with a hospital to 'optimise physician productivity' and 'reduce average length of stay,' those are legitimate operational goals. But they are also goals that, pursued without counterbalancing patient advocacy, can reduce the time a doctor has for actual communication — the kind that builds trust, reduces anxiety, and improves outcomes.
Shorter length of stay is good for ARPOB. It is not always good for the patient who needed one more day of monitoring.
A note on what PE does do well
It would be lazy to paint this as purely a story of predatory capital versus innocent patients. The reality is more mixed.
India has a genuine healthcare access problem. Bed density in Tier 2 and Tier 3 cities is 0.8–1.2 per 1,000 people, compared to 2.7–3.0 in metros. PE capital has funded expansion into underserved geographies that government and charitable healthcare could not reach. It has modernised billing, reduced infection rates through standardised protocols, and professionalised HR practices in hospitals that previously treated nurses as exploitable labour.
THE HONEST CREDIT
A well-run PE-backed hospital chain with clear ethical guardrails can genuinely be better than the chronically underfunded charitable hospital or the single-doctor nursing home with no accountability structures.
The problem is not PE itself. The problem is the absence of a counterweight.
What PE does not naturally bring — what must come from regulators, patient advocacy groups, and a more health-literate public — is a commitment to communication that prioritises patient understanding over patient conversion.
What should you actually do with this?
The most practical takeaway isn't cynicism. It is a specific kind of literacy.
When a PE-backed hospital sends you a health package offer, ask whether it's triggered by your clinical history or by a marketing segment you've been placed in. When you're offered a premium room upgrade during admission, understand that the person making the offer works within a revenue incentive structure. When a follow-up consultation is recommended, ask your doctor whether it is clinically necessary — and notice whether they hesitate before answering.
None of this means the hospital is lying to you. Most doctors in these systems are operating with genuine clinical integrity, often against structural pressure. But they are working inside a process that has been designed — at the organisational level — to optimise for metrics.
