

My first exposure to conversations about mental health did not happen in a clinic or a classroom. It happened on online forums, long Reddit threads and late-night Discord servers, where strangers spoke about their minds with honesty and freedom from judgment that conversations rarely allowed. The posts often began with a diagnosis and ended with uncertainty.
“I got diagnosed with ADHD last week and I don’t know how to feel about it yet.”
“Some people say it explains everything about them. I’m not sure it explains me.”
“Is this actually what this disorder is like? Everything I read online sounds different.”
Reading through these conversations felt like watching hundreds of people trying to understand what a single clinical word meant. A diagnosis appeared in these threads as both explanation and question. For some, it felt like clarity; for others, it created uncertainty about identity and treatment.
None of these conversations were rooted in clinical research. They came from confusion, relief, curiosity, and the desire to make sense of one’s mind. In research language, we call this lived experience.
Late at night, when these questions feel louder, you type symptoms into Google- fatigue, inability to focus, constant overwhelm. The search results rarely begin with research papers, but with videos promising to translate complex experiences into something understandable. But lived experience resists that kind of simplification, and my instinct as a researcher pushed the search further.
Soon I found myself on PubMed and Google Scholar, reading papers about SSRIs, diagnostic criteria for bipolar disorder, and the overlap between autism and ADHD. Each article offered a different interpretation of the same behaviours- some emphasizing neurobiology, others thresholds or treatment outcomes.The literature revealed how much work goes into defining mental health conditions.
Gradually, clinical terms begin to circulate around lived experience.Words that once seemed confined to medical journals start appearing in everyday conversations. A diagnosis travels across scientific research, clinical practice and everyday conversations.
Exchanges shape expectations.
Much of this knowledge travels informally in fragments: a friend’s story, a recommendation shared over coffee, a discussion thread online. In conversations, someone recalls a therapist who listened with care, while another describes a consultation that felt compressed into a few minutes. As you move through research, clinical encounters, and everyday conversations, the meaning of a diagnosis begins to shift, each context quietly reshaping how it is understood.
For a science communicator writing about mental health, this creates a unique responsibility.
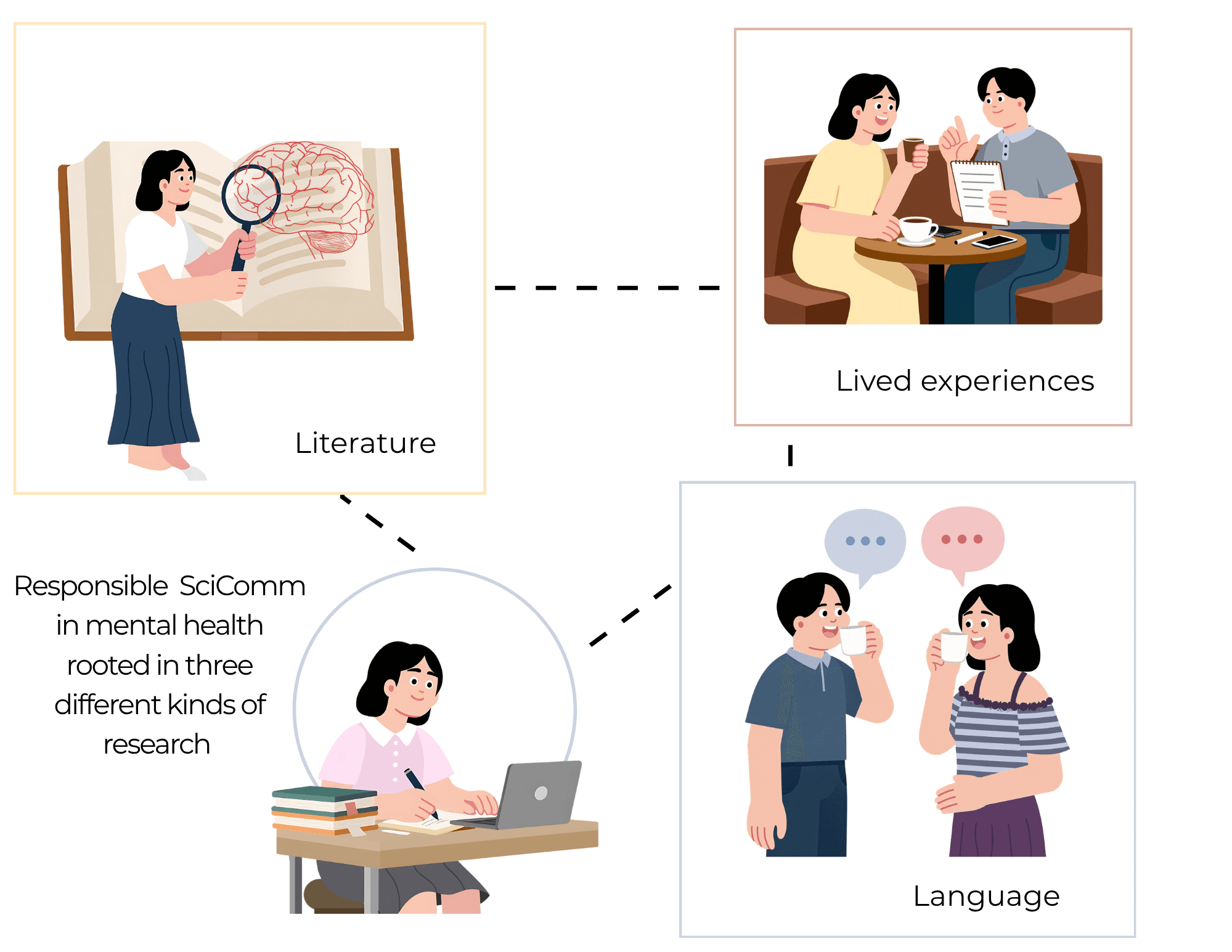
Responsible science communication often happens at the intersection of three elements threaded together: scientific evidence, lived experience- both your own and that of others and the language used to translate between them.
Scientific literature provides the foundation. It explains how clinicians identify patterns of symptoms, how treatments are evaluated, and how researchers study the brain. Without this evidence, mental health writing risks becoming speculation or misinformation.
You find yourself moving between different kinds of knowledge. On one side are research papers, diagnostic criteria, and clinical studies that describe patterns of symptoms with precision. On another are the lived experiences of people, about their own lives, how a diagnosis felt, how it reshaped the way they understood their past relationships, trauma, school life, upbringing or how symptoms appear differently across individuals.
Connecting these spaces is language.
It's crucial to remember that the words chosen to describe mental health shape how diagnoses travel from scientific research into public understanding. Language can clarify complex ideas, but it can also oversimplify them. A diagnosis can become a helpful framework, or it can become a rigid label that defines a person too narrowly.
As a science communicator, I often think of the task as holding complexity in view rather than smoothing it away. Mental health diagnoses sit inside scientific models that are constantly evolving, shaped by new research, clinical practice, and debate. Writing about them therefore requires acknowledging that our understanding of the brain is still incomplete but developing. At the same time, it means paying attention to the stories people tell about their own lives- how a diagnosis entered their narrative, what it helped explain, and what questions it left behind. I often find it useful to make notes of these experiences and place them alongside what I encounter in the scientific literature. Reading across different sources helps situate personal accounts within the broader landscape of research and emerging clinical understanding.
Another responsibility lies in how we explain these ideas.
I often use analogies to make complex research more accessible. Scientific explanations frequently rely on technical language that can feel distant from everyday experience. Analogies provide a way of connecting unfamiliar concepts to things people understand.
For example, attention regulation in ADHD is sometimes described as a difference in how the brain filters incoming information. One way to illustrate this is to imagine a radio trying to tune into a single station while several signals play at once. The radio is not broken. It simply receives more signals than it can easily filter. The analogy does not capture every aspect of neurobiology, but it offers an intuitive way to understand the experience of competing attention.
Analogies like these become tools for responsible, research-based science communication. They help readers approach complex ideas without stripping away nuance.
Visual illustrations can play a similar role.
Many science communicators use conceptual illustrations to show relationships that are difficult to describe with words alone.
In my work, illustrations often emerge from the same places where conversations about mental health began. Online communities, personal stories, and everyday language. A visual idea might come from a metaphor someone used to describe their experience, or from a pattern that appears repeatedly in discussions about attention, mood, or memory. For instance, people with anxiety often describe a sense of constant anticipation, as if something is about to go wrong. Visually, this might take the form of a notification that never disappears, lingering on the screen and repeatedly drawing attention back, even when nothing new has happened. In this way, illustrations help make research intuitive. My favorite analogies in neuroscience come from my everyday life. For instance, I once wrote a blog about Taylor Swift’s August and how the song captures something fundamental about episodic memory. The way personal moments are revisited and quietly reshaped each time they are remembered.
Finally, responsible communication also depends on how we refer to people themselves.
Small shifts in language can significantly shape perception. Person-first language, such as saying “a person with schizophrenia” rather than “a schizophrenic person”, keeps the individual at the center and the diagnosis as only one aspect of their identity.
These linguistic choices may seem minor, but they influence how readers conceptualize mental health and how stigma is reinforced or challenged.
Writing about mental health responsibly involves more than summarizing scientific findings. It requires careful attention to evidence, language, and lived experience. It asks communicators to explain research clearly while respecting the complexity of the people whose lives intersect with these diagnoses.
Mental health diagnoses begin as clinical categories, but in everyday life they often turn into stories people use to interpret their experiences.
The role of a science communicator is to keep these stories grounded in evidence while leaving room for what science has yet to explain.

